





Hair thinning and balding aren’t just concerns that come with age—they can also be written in your genes. Whether you’re noticing a receding hairline, thinning crown, or overall hair shedding, your DNA may play a key role in shaping your scalp’s future.
Fortunately, understanding your inherited hair pattern gives you a critical opportunity: you can act early and protect the hair you have.
Below, we break down the science behind genetic hair loss and what you can do if your DNA points to a higher risk of pattern baldness.
What Is Pattern Baldness?
Pattern baldness—also known as androgenetic alopecia—is the most common form of hair loss in both men and women. In men, it often starts with temple recession and progresses to more extensive scalp exposure over time. In women, it typically appears as diffuse thinning on the crown, with the hairline generally staying intact.
While the progression and presentation differ by gender, the root cause is similar: sensitivity to dihydrotestosterone (DHT), a hormone that can shrink hair follicles and shorten the hair growth cycle. Genetic variations can influence how sensitive your follicles are to DHT, how your body metabolizes key nutrients, and how quickly hair loss may progress.
Inherited Stages of Hair Loss
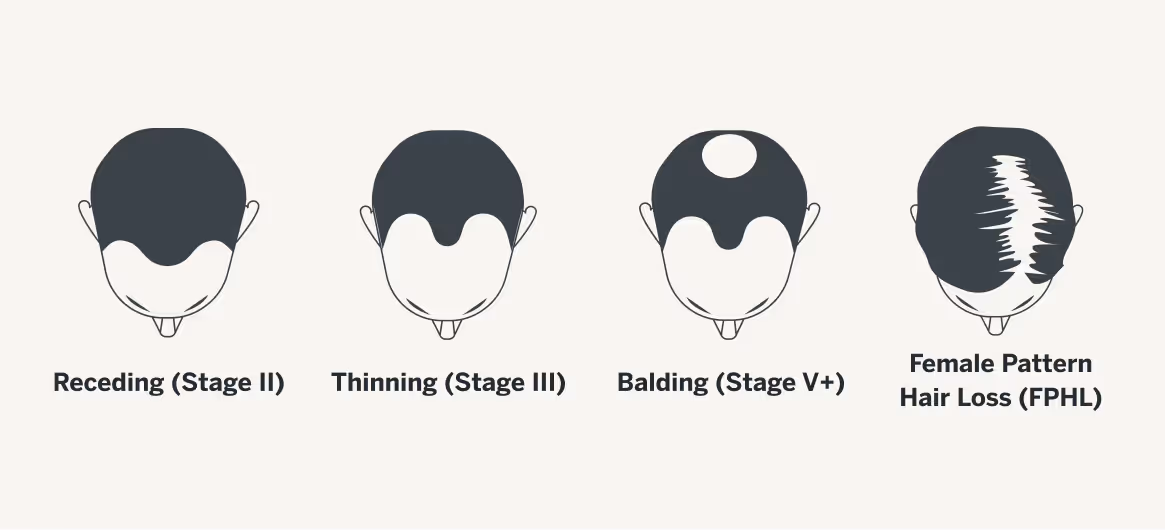
If your DNA shows a low risk for androgenetic alopecia, you may still notice subtle signs like temple thinning or mild crown reduction. That’s why early detection and preventive care are essential. Below, we discuss risk levels and treatment recommendations based upon the Norwood-Hamilton Scale (also referred to as simply Norwood).
This widely used classification system measures the stages of male pattern baldness, ranging from minimal hairline recession (Stage I) to extensive hair loss affecting most of the scalp (Stage VII). It helps clinicians track progression, guide treatment decisions, and compare hair loss patterns over time.
A. Receding Hairline (Norwood Stage II – Moderate Androgenetic Alopecia)
If your StrandIQ™ analysis finds that you are in the earlier stages of hair loss, a balanced plan focused on prevention, mild growth stimulation, and scalp health can help maintain existing density. Moderate interventions work best for those with minimal thinning who want to get ahead of further loss.
Treatment Approach:
- Low Risk:
Even with a low genetic predisposition, early intervention helps preserve long-term hair health and delay future thinning:
- Minimize heat styling and harsh chemical treatments; massage scalp gently to promote circulation.
- Ensure adequate intake of essential nutrients like omega-3s, iron, zinc, and protein.
- Prioritize mental wellness and sleep quality to regulate hair-growth hormones.
- Schedule occasional dermatologist visits to document hair density and catch potential changes early.
- Moderate Risk:
If you're at moderate genetic risk and noticing early signs of loss (e.g., thinning part or slower regrowth), now is the time to reinforce scalp and follicle health:
- Begin over-the-counter minoxidil or mild botanical DHT blockers to help maintain or improve density.
- Use volumizing, sulfate-free shampoos and lightweight conditioners designed for thinning hair.
- Focus on nutrition (iron, vitamin D, biotin), regular exercise, and reducing stress to help stabilize hormonal fluctuations.
- Track progress monthly with photos and scalp exams; consult a Happy Head dermatologist every 6–12 months for evaluation and escalation if needed.
- High Risk:
Individuals at high risk should take early, targeted action to prevent rapid progression:
- Start DHT blockers such as finasteride and dutasteride (for men) or spironolactone/anti-androgens (for women) under medical supervision.
- Use topical minoxidil (5% for men, 2% or 5% for women) to support regrowth and maintain density.
- Consider PRP (Platelet-Rich Plasma) or low-level laser therapy for added support.
- Adopt a nutrient-dense, protein-rich diet, maintain scalp hygiene, manage stress, and get quality sleep.
- Partner with a Happy Head dermatologist to create a long-term, personalized treatment plan.
B. Vertex Thinning (Norwood Stage III–IV – Advanced Vertex Androgenetic Alopecia)
For individuals experiencing noticeable thinning but still maintaining some follicle activity, targeted therapies can help slow progression and restore density. These approaches go beyond basic prevention, incorporating clinically validated topical and oral treatments alongside specialized scalp care.
Treatment Approach:
- Low Risk:
For individuals with slower progression:- Emphasis is on preventive care—prioritize a diet rich in vitamins, protein, antioxidants, and adequate hydration.
- Support routines like exercise, stress relief, and quality sleep.
- Schedule routine dermatologist check-ups to catch subtle changes early.
- Moderate Risk:
For those with noticeable vertex thinning, use a dual approach:
- High Risk:
Individuals with rapid, pronounced hair loss at both temples and crown need an aggressive, multi-pronged strategy:
- Start prescription finasteride or mild botanical DHT blockers and continue topical treatments.
- Explore advanced therapies like PRP (Platelet-Rich Plasma) and hair transplantation.
- Combine with a nutrient-rich diet, regular exercise, stress management, and scalp health monitoring.
C. Extensive Balding (Norwood Stage V+ – Severe Androgenetic Alopecia)
When hair loss is advanced or progressing rapidly, or if your StrandIQ™ report finds that you are at risk for extensive balding, a more aggressive and comprehensive approach may be necessary. This level of care often combines prescription medications, in-office procedures, and supportive scalp therapies to maximize follicle preservation and regrowth potential.
Treatment Approach:
- Low Risk:
For those with low genetic risk of severe balding:
- Continue preventive practices—balanced nutrition, hydration, stress management, and good sleep.
- Keep up regular dermatological check-ins to detect any early signs and intervene promptly.
- Moderate Risk:
With moderate progression into severe baldness:
- Maintain hair health with specialized shampoos, conditioners, and OTC treatments like minoxidil.
- Consult with your Happy Head dermatologist for progress tracking and possible prescription additions.
- Support with antioxidant-rich diet and lifestyle modifications to bolster scalp resilience.
- High Risk:
Rapid and extensive hair loss necessitates immediate and comprehensive intervention:- Combine healthy lifestyle habits and mild botanical DHT blockers with professional treatments like finasteride, minoxidil, PRP, or hair transplant.
- Use a multidisciplinary approach—dermatologic care, nutritional support, and stress management—to manage both hair and overall well-being.
Understanding Female Pattern Balding
Female pattern hair loss (FPHL) is the most common form of progressive hair thinning in women, often linked to genetic predisposition, hormonal fluctuations, and changes in follicle sensitivity with age. Unlike male pattern baldness, which frequently begins with a receding hairline or distinct bald spots, FPHL tends to cause diffuse thinning over the crown while the frontal hairline remains intact. Because hair loss at this stage can accelerate over time, early detection and a personalized treatment plan are essential to preserving hair density and preventing further miniaturization of follicles.
Low Likelihood – Focus on Prevention and Scalp Health
If your StrandIQ™ analysis shows that you are at a lower genetic predisposition for FPHL, proactive scalp and follicle care can still help maintain hair density as you age.
- Optimize your scalp health
Use gentle, sulfate-free shampoos and exfoliating treatments once or twice a month to keep follicles clear. - Eat a nutrient-rich diet
Prioritize foods with iron, zinc, biotin, and omega-3s to nourish hair from the inside out. - Protect hair from UV and heat
Shield hair from excessive sun exposure and avoid high-heat styling tools to minimize stress on follicles.
Moderate Likelihood – Combine Maintenance with Targeted Support
With a moderate genetic predisposition, you may benefit from adding targeted hair growth support to your routine alongside healthy scalp habits.
- Add growth-boosting topicals
Consider over-the-counter minoxidil to stimulate follicles and slow shedding. - Layer serums into your routine
Support circulation and follicle activity with scientifically backed scalp serums. - Hormonal Health Check
Speak with your doctor about underlying hormonal shifts, especially during perimenopause or menopause.
High Likelihood – Implement a Proactive, Multi-Layered Plan
A strong genetic predisposition to FPHL often requires a more aggressive, consistent regimen to slow or halt progression.
- Consider medical interventions
Discuss prescription treatments like oral spironolactone, finasteride, or low-dose oral minoxidil with your Happy Head physician. - Advanced scalp therapies
Consider in-office options like platelet-rich plasma (PRP) therapy or low-level laser therapy (LLLT). - Combine products
Use a mix of topical growth stimulants, anti-androgen therapy, and lifestyle modifications for maximum follicle preservation.
How Male and Female Pattern Baldness Differs
While men typically experience a more recognizable pattern—starting at the hairline or crown—women often deal with gradual thinning that spreads over a wider area. In both cases, hair follicles become smaller, producing shorter, thinner strands until growth stops altogether.
Genetics play a major role, but hormones, stress, nutrition, and medical conditions can all amplify the rate of hair loss. That’s why understanding your genetic tendencies is so powerful: it allows for personalized, preventive strategies.
Genetics Aren’t Destiny
While your DNA may influence how likely you are to experience pattern baldness, it doesn’t guarantee it will happen. By understanding your inherited hair pattern, you gain a roadmap to act early, adjust your care routines, and protect your scalp health before visible signs of hair loss appear.
Resources
StrandIQ SNP Marker Count:
- Male Balding Pattern A: 39
- Male Balding Pattern B: 33
- Male Balding Pattern C: 44
- Female Pattern Hair Loss: 4
StrandIQ Genes for Trait:
- Male Balding Pattern A:
C10orf11, CCDC140, CEP112, CLYBL, CPEB2-AS1, EPC1, EYA4, FARSB, FGF5, GLIS1, GLIS3, GORAB, HDAC9, JAZF1, LGR4, LINC00536, LINC00578, MRPS22, NSF, PAX3, PCCA, PRDM6, PRKCH, RAD51B, RP1-283K11.3, RP1-79C4.1, RP11-125P18.1, RP11-15B24.5, RP11-346D6.6, RP11-66B24.5, RP11-84D1.2, RREB1, RUNX1, SGPP2, SHFM1, TCF12, TEX41, ZBTB20, ZBTB20-AS1 - Male Balding Pattern B:
AC004870.3, AC004870.4, AC004901.1, AC097468.7, AC217772.1, C10orf11, C1orf127, DPY30, EBF1, EPC1, FGF5, HDAC9, KANSL1, LHPP, MEMO1, MRPS22, OFCC1, PAX3, PDGFA, PRDM6, RP11-283G6.4, RP11-283G6.5, RP11-542A14.1, RP11-846C15.2, RSPO2, RUNX1, SLC14A2, SSPN, TBX15, TEX41, WARS2, WNT10A, ZHX3 - Male Balding Pattern C:
AC003070.1, AC010987.5, AC092162.1, ALDH1L1-AS2, ARHGAP27, BCKDHA, C10orf11, C1orf127, CASC15, CTC-435M10.3, DPY30, EBF1, FAM53B, FGF5, HDAC9, KLF15, LHPP, LINC00670, LRRC36, MEMO1, MRPS22, NSF, OFCC1, PRDM6, RP11-12J10.3, RP11-283G6.4, RP11-283G6.5, RP11-418J17.1, RP11-576I22.2, RP11-846C15.2, RP11-84D1.2, RP4-799D16.1, RSPO2, RUNX1, RUNX3, SLC14A2, SPAG17, SSPN, TBX15, TEX41, TWIST1, WARS2, ZBTB38, ZHX3 - Female Pattern Hair Loss:
CYP19A1, ESR2, VDR, HSD3B1
References:
Male Balding Patterns
Backman, J.D., et al. (2021). Exome sequencing and analysis of 454,787 UK Biobank participants. Nature, 599(7886), 628–634. PMID: 34662886.
Chen, Y., et al. (2023). Genetic prediction of male pattern baldness based on large independent datasets. European Journal of Human Genetics, 31(3), 321–328. PMID: 36336714.
Eriksson, A.L., et al. (2009). Genetic variations in sex steroid-related genes as predictors of serum estrogen levels in men. Journal of Clinical Endocrinology & Metabolism, 94(3), 1033–1041. PMID: 19116238.
Hagenaars, S.P., et al. (2017). Genetic prediction of male pattern baldness. PLoS Genetics, 13(2), e1006594. PMID: 28196072.
Heilmann-Heimbach, S., et al. (2017). Meta-analysis identifies novel risk loci and yields systematic insights into the biology of male-pattern baldness. Nature Communications, 8, 14694. PMID: 28272467.
Kanda, S., et al. (2015). Effects of functional genetic polymorphisms in the CYP19A1 gene on prostate cancer risk and survival. International Journal of Cancer, 136(1), 74–82. PMID: 24803183.
Liu, F., et al. (2016). Prediction of male-pattern baldness from genotypes. European Journal of Human Genetics, 24(6), 895–902. PMID: 26508577.
Marcińska, M., et al. (2015). Evaluation of DNA variants associated with androgenetic alopecia and their potential to predict male pattern baldness. PLoS One, 10(5), e0127852. PMID: 26001114.
Pirastu, N., et al. (2017). GWAS for male-pattern baldness identifies 71 susceptibility loci explaining 38% of the risk. Nature Communications, 8(1), 1584. PMID: 29146897.
Yap, C.X., et al. (2018). Dissection of genetic variation and evidence for pleiotropy in male pattern baldness. Nature Communications, 9(1), 5407. PMID: 30573740.
Female Pattern Hair Loss
Ho, C-Y., et al. (2023). Female pattern hair loss: An overview with focus on the genetics. Genes, 14(7), 1326. PMID: 37510231.
Łukasik, A., et al. (2022). The role of CYP19A1 and ESR2 gene polymorphisms in female androgenetic alopecia in the Polish population. Postepy Dermatologii i Alergologii, 39(4), 708–713. PMID: 36090736.
Redler, S., et al. (2017). Genetics and other factors in the aetiology of female pattern hair loss. Experimental Dermatology, 26(6), 510–517. PMID: 28453904.
Rui, W., et al. (2015). Association of single nucleotide polymorphisms in the CYP19A1 gene with female pattern hair loss in a Chinese population. Dermatology, 231(3), 239–244. PMID: 26228318.
Seleit, I., et al. (2020). Vitamin D receptor gene polymorphisms Taq-1 and Cdx-1 in female pattern hair loss. Indian Journal of Dermatology, 65(4), 259–264. PMID: 32831364.
Tu, Y.A., et al. (2019). HSD3B1 gene polymorphism and female pattern hair loss in women with polycystic ovary syndrome. Journal of the Formosan Medical Association, 118(8), 1225–1231. PMID: 31056381.
Yip, L., et al. (2009). Gene-wide association study between the aromatase gene (CYP19A1) and female pattern hair loss. British Journal of Dermatology, 161(2), 289–294. PMID: 19438456.
This content, including StrandIQ™ DNA analysis reports and any Happy Head products and/or services referenced therein, is for informational and cosmetic purposes only. It is not intended to diagnose, treat, cure, or prevent any disease. This content does not constitute medical advice and should not be used to make healthcare decisions. References to prescription treatments are educational in nature. Always consult a licensed healthcare professional for any medical concerns or treatment decisions.



.avif)

